PATIENT APPOINTMENT RECORD (Sample)
🗂️ Patient Appointment Record Form
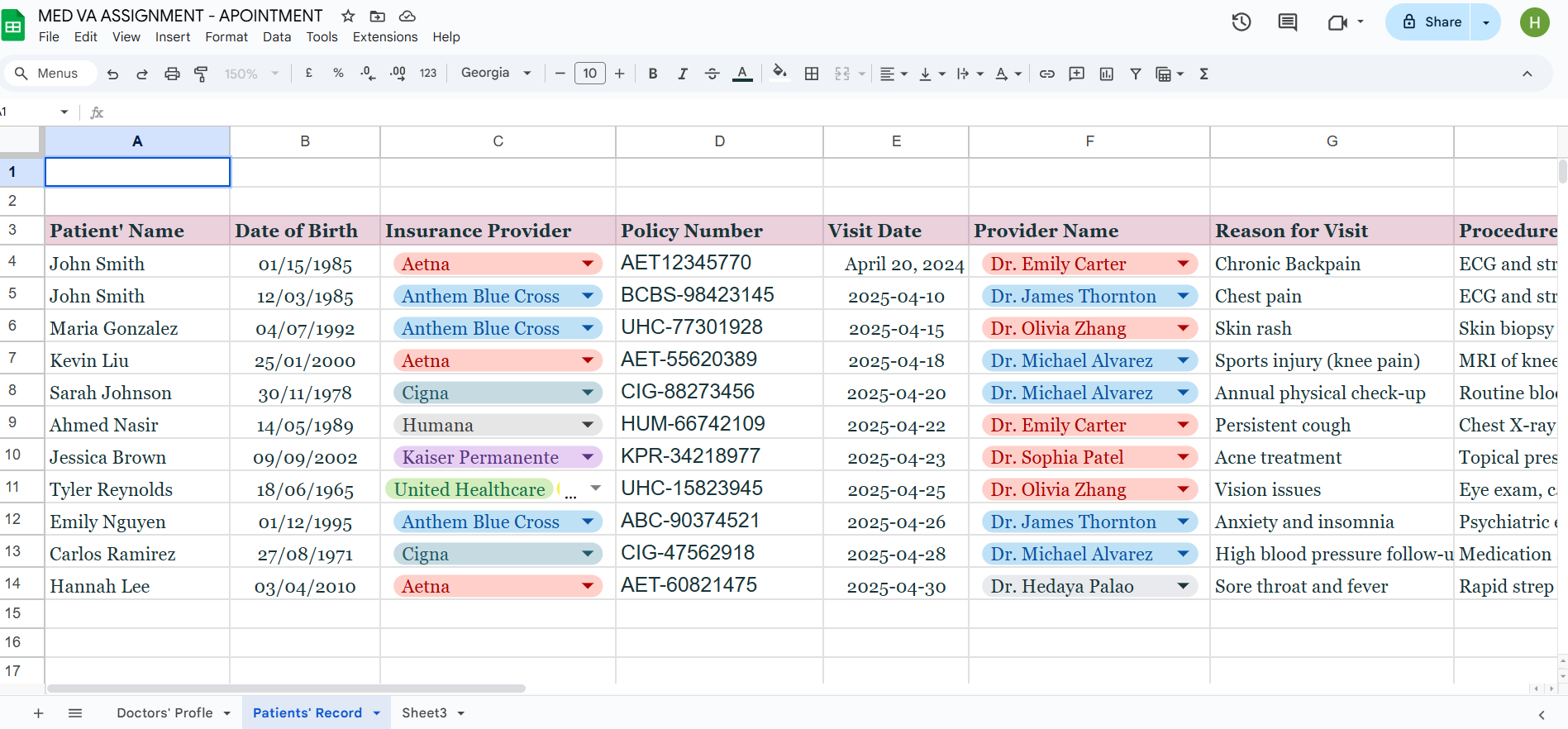
1. Patient Information
| Full Name | ___________________________________ |
| Date of Birth | ___________________________________ |
| Gender | ☐ Male ☐ Female ☐ Other |
| Contact Number | ___________________________________ |
| Email Address | ___________________________________ |
| Address | ___________________________________ |
2. Insurance Information
| Insurance Provider | ___________________________________ |
| Policy Number | ___________________________________ |
| Coverage Type | ☐ HMO ☐ PPO ☐ Medicare ☐ Medicaid ☐ Other: __________ |
| Coverage Validity | ____________ to ____________ |
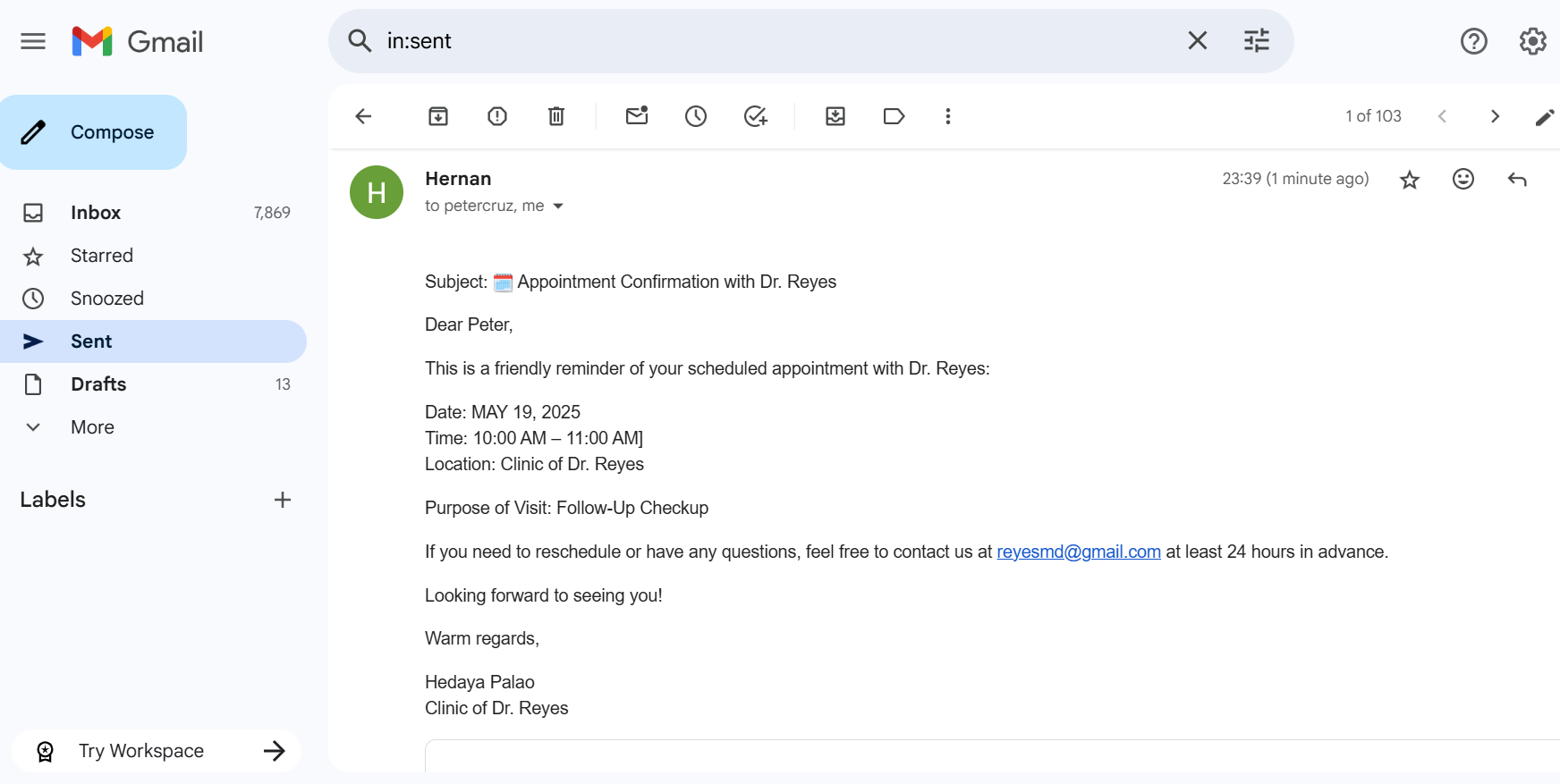
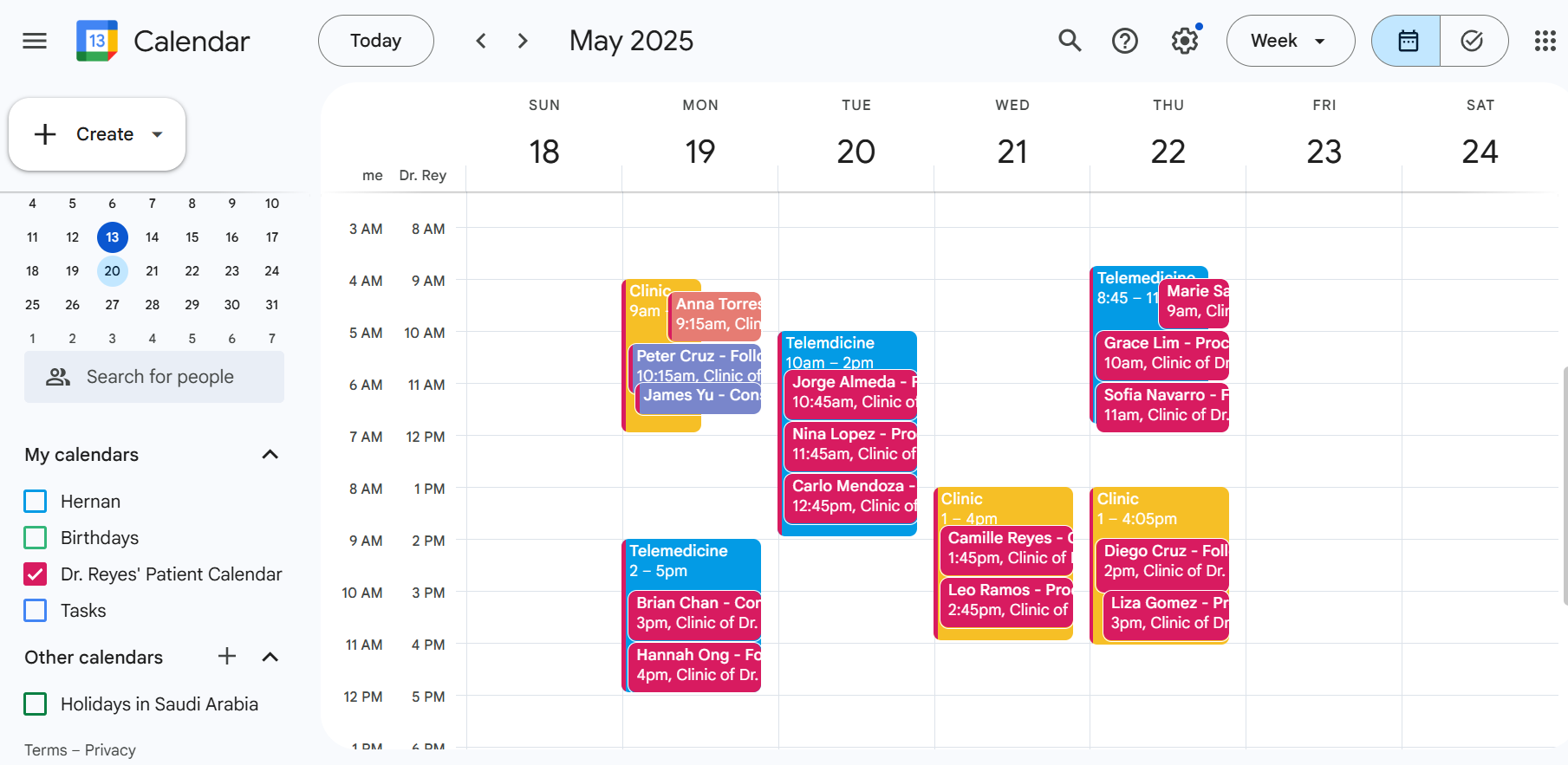
3. Appointment Details
| Visit Date | ___________________________________ |
| Visit Type | ☐ Initial ☐ Follow-up ☐ Routine ☐ Emergency |
| Referring Physician | ___________________________________ |
| Department | ___________________________________ |
4. Reason for Visit
Chief Complaint / Symptoms:
Onset Date: ______________________
Severity: ☐ Mild ☐ Moderate ☐ Severe
Other Symptoms: _________________________________________________________________
5. Vitals & Clinical Notes
| Blood Pressure | ___________________ |
| Heart Rate | ___________________ |
| Temperature | ___________________ |
| Respiratory Rate | ___________________ |
Clinical Observations:
6. Procedures Performed
| ____________________________________ | __________ |
| ____________________________________ | __________ |
| ____________________________________ | __________ |
7. Prescriptions & Recommendations
Medications Prescribed:
Tests Ordered / Follow-Up Plans:
8. Provider Information
| Attending Physician | ___________________________________ |
| NPI Number | ___________________________________ |
| Clinic / Hospital | ___________________________________ |
| Contact Info | ___________________________________ |